- Home
- About Journals
-
Information for Authors/ReviewersEditorial Policies
Publication Fee
Publication Cycle - Process Flowchart
Online Manuscript Submission and Tracking System
Publishing Ethics and Rectitude
Authorship
Author Benefits
Reviewer Guidelines
Guest Editor Guidelines
Peer Review Workflow
Quick Track Option
Copyediting Services
Bentham Open Membership
Bentham Open Advisory Board
Archiving Policies
Fabricating and Stating False Information
Post Publication Discussions and Corrections
Editorial Management
Advertise With Us
Funding Agencies
Rate List
Kudos
General FAQs
Special Fee Waivers and Discounts
- Contact
- Help
- About Us
- Search


The Open Biomaterials Journal
(Discontinued)
ISSN: 1876-5025 ― Volume 5, 2014
Preliminary Evaluation of Six Current Bilirubin Adsorbents on Potential Application for the Hemoperfusion of Severe Neonatal Jaundice
Kai_Wang Ma*, Shu_Ying Feng , Jian_Ying Yang
Abstract
Background:
Now hemoperfusion has not been used for the treatment of severe neonatal jaundice, and bilirubin adsorbent with high adsorption and safety should be the prerequisite for the use.
Objectives:
To investigate the adsorption of six kinds of current adult/industrial bilirubin adsorbents from severe neonatal jaundice plasma, then screen the best one with highest adsorption for further evaluations, with an aim to provide preliminary experimental reference for the potential clinical use of hemoperfusion in newborn.
Methods:
Six kinds of current bilirubin adsorbents [NKA-9, NK-110, polymethacrylic acid (PMMA), polyvinyl alcohol (PVA), chitosan and burning resin] were selected for the investigation. Under the proportion of 1 portion of adsorbent (g) to 2 portion of severe neonatal jaundice plasma (ml), the adsorbent was allowed to dynamically contact the plasma (recycled from the discarded plasma of severe neonatal jaundice inpatients after exchange transfusion treatment) at 37°C for 1 h respectively, then their adsorption for bilirubin was calculated and compared, and then based on the comparative result, the adsorbent with best adsorption was subject to further evaluation such as its effect on the blood elements, the hemolysis system and blood clotting system of newborn.
Results:
Under the same test conditions, the adsorption of NKA-9 for bilirubin was the best and up to 85%, and its effect on other physiological indexes was clinically acceptable.
Conclusion:
The preliminary evaluations offer us the knowledge and reference of hemoperfusion therapy being potentially applied in the treatment of severe neonatal jaundice, as well as other shortcomings existing within the therapy to be overcome.
Article Information
Identifiers and Pagination:
Year: 2010Volume: 2
First Page: 53
Last Page: 57
Publisher Id: TOBIOMTJ-2-53
DOI: 10.2174/1876502501002010053
Article History:
Received Date: 17/10/2009Revision Received Date: 15/1/2010
Acceptance Date: 20/1/2010
Electronic publication date: 1/9/2010
Collection year: 2010
open-access license: This is an open access article licensed under the terms of the Creative Commons Attribution Non-Commercial License (http: //creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted, non-commercial use, distribution and reproduction in any medium, provided the work is properly cited.
* Address correspondence to this author at the College of Medical technology and Engineering, Henan University of Science and Technology, Luoyang, 471003, PR China; E-mail: mkw007@126.com
| Open Peer Review Details | |||
|---|---|---|---|
| Manuscript submitted on 17-10-2009 |
Original Manuscript | Preliminary Evaluation of Six Current Bilirubin Adsorbents on Potential Application for the Hemoperfusion of Severe Neonatal Jaundice | |
1. INTRODUCTION
For the newborns, neonatal jaundice is the common disease [1]. There are two types of neonatal jaundice: one is physiological and the other is pathological. As for the physiological, it can be automatically recovered without any treatments. Whereas, for the pathological, it falls into three types: mild, moderate and severe. If they were not to be properly or promptly handled (esp. the severe one), it can cause kernicterus, and consequently sequela or even death may occur [2]. The pathogeny of neonatal jaundice [2] is that the amount of bilirubin overproduces so that it is beyond the excretive and metabolic capability of the neonatal body, thus results in the accumulation of redundant bilirubin. Therefore, the treatment should be based on how to reduce the level of bilirubin effectively and quickly. Now, three clinical thera-pies [3-5] (drug, blue phototherapy and exchange trans-fusion) are in use for the treatment. Drug can accelerate the excretive and metabolic process of bilirubin; however, it is now seldom used in clinic due to its great side effect [6]. Blue phototherapy can change the excretive and metabolic pathway of bilirubin, which is only suitable for mild sick neonatal but also has side effect [7-8]. Exchange transfusion is now the last resort for the treatment of severe neonatal jaundice, in which there are some disadvantages, such as blood cross-infection, scarcity of blood source and operation complexity [9-10]. Because the incidence of severe neonatal jaundice is in rise [1,11] and there exist some larvaceous disadvantages to be overcome for the exchange transfusion, in view of high safety, there is an imminent demand to develop a new, safer, more economic and simple treatment for severe neonatal jaundice to substitute exchange transfusion.
Hemoperfusion [4,12-13] has been clinically used since 1970s, whose characteristics are to clear pathogenic material directly and quickly from blood or plasma so as to purify the blood, and whose key depends on the perfusion adsorbent with high specificity and adsorption as well as good hemocompatibility [14-16]. Therefore, hemoperfusion has the potentiality to substitute exchange transfusion for the treatment of severe neonatal jaundice. Because of the newborn physiological particularity, the key to apply the hemoperfusion for the treatment depends on whether the bilirubin adsorbent is of high specificity, high adsorption and good hemocompatibility for the newborn blood. Now, several bilirubin adsorbents have been reported, such as NKA-9 [17], NK-110 [17], PVA [17], PMMA [18], chitosan [19] and burning resin [20], which are mainly used in industry to extract bilirubin or in clinic for adult hyperbilirubinemia hemoperfusion [21]. But within our knowledge, there is no report about their use in the hemoperfusion for severe neonatal jaundice and on their adsorption for bilirubin from severe neonatal jaundice plasma/blood. This study was aimed to test their adsorption properties upon neonatal jaundice plasma, and then screen out the best for further evaluation, with an aim to provide clinical experimental reference for the choice or development of bilirubin adsorbent for the hemoperfusion in severe neonatal jaundice.
2. MATERIALS AND METHODS
2.1. Main Materials and Equipments
Blood/plasma was obtained from newborn in patients with severe jaundice in the Chongqing Children's Hospital, China, and the blood/plasma were those that were recycled from the discarded blood/plasma of severe neonatal jaundice inpatients after exchange transfusion treatment; three bilirubin adsorbent candidates (NKA-9, NK-110 and PMMA) were provided from chemical plant of Nan_Kai University China; three bilirubin adsorbent candidates (PVA, chitosan and charring resin) were provided by Tianjin Jinlin Biochemical Development Company China. Coagulometer (CA1500, USA), Electrolyte Analyzer (XD685, USA), Automatic Biochemical Analyzer (Dimension RXL, USA), Blood Gas Analyzer (Bayer-860, USA), Specific Protein Detector (Nephster, Germany), Hemoperfusion Device (self-made). (Note: NKA-9 and NK-110 are a kind of macroporous resin).
2.2. Adsorption of the Candidates from Severe Neonatal Jaundice Plasma
The adsorbent (15 g) was filled into the hemoperfusion column. The initial value of bilirubin level in the severe neonatal jaundice plasma was firstly assayed, then 30ml the plasma was allowed to circulate through the hemoperfusion column for 1h at 37C. Finally the end value of bilirubin level was assayed after the circulations. With the same procedure and conditions, the rest were subjected to the same treatment respectively, and the one with best adsorption was screened out for further evaluation.
2.3. Further Evaluations of NKA-9
From section 2.2, NKA-9 did the best among the six; therefore, it was screened out for further evaluation.
2.3.1. The Effects of NKA-9 on the Plasma Components of Severe Neonatal Jaundice
7g NKA-9 was filled in the hemoperfusion column, then 14 mL severe neonatal jaundice plasma was allowed to circulate through the column at 37C for 1 h. Those biochemical indicators, such as plasma protein, indicators of renal function, inorganic ions, immune system, enzyme system and auxiliary system, were assayed before and after the circulation to investigate its effects on the blood elements and components.
2.3.2. Effects of NKA-9 on the Coagulation System of Severe Jaundice Neonatal
7g of NKA-9 was filled in the hemoperfusion column, then 14 mL severe neonatal jaundice plasma anticoagulated with 1:9 sodium citrate anticoagulant was allowed to circulate through the column at 37C for 1 h. Those indicators of coagulation system, such as prothrombin time (PT), activated partial thromboplastin time (APTT), fibrinogen (FIB) and prothrombin time (TT) were assayed before and after the circulation with CA1500. Similarly, 7g NKA-9 was filled in the hemoperfusion column, then 14 mL severe neonatal jaundice plasma anticoagulated with heparin anticoagulant was allowed to circulate through the column at 37C for 1 h, then Complement indicator (C3) was assayed before and after the circulation with CA1500.
2.3.3. Effects of NKA-9 on the Hemolytic System of Severe Jaundice Neonatal
7g NKA-9 was filled in the hemoperfusion column; 10mL out of 120 mL severe neonatal jaundice blood was taken for blank test, and 110 mL of the rest was divided into halves equally to separate plasma and blood cells respectively. The blood cells just isolated were temporarily preserved respectively. One portion of the plasma was allowed to circulate through the column at 37°C for 1h, whereas the other without circulation was as the control. After the circulation, the two portions of plasma were mixed with the original corresponding blood cells isolated respectively, and then the hemolytic indicators of the original, the treated and the untreated blood were measured respectively, such as red blood cells, hemoglobin, the average red cell volume, platelet count, WBC, the average amount of hemoglobin, hematocrit, mean hemoglobin concentration, erythrocyte distribution width, mean platelet volume, the absolute value of lymphocytes, neutrophils absolute, absolute value of intermediate cells, percentage of lymphocytes and neutrophilic leukocyte.
3. RESULTS
3.1. Adsorption of Six Bilirubin Adsorbent Candidates from Severe Neonatal Jaundice Plasma
Under the experimental conditions, their adsorptive capability was shown in Fig. (1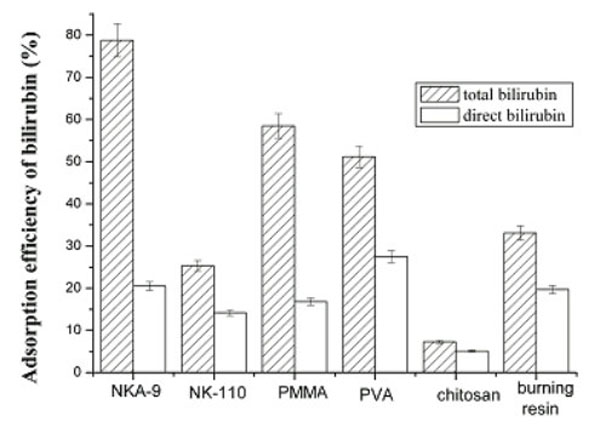 ). We can see NKA-9, PVA and burning resin had good adsorption for direct bilirubin (DB), among them, PVA ranked the top. NKA-9, PMMA resin and PVA had good adsorption for total bilirubin (TB), among them, NKA-9 ranked the top. Taken together, we considered the NKA-9 had the best adsorption for bilirubin from severe neonatal jaundice plasma.
). We can see NKA-9, PVA and burning resin had good adsorption for direct bilirubin (DB), among them, PVA ranked the top. NKA-9, PMMA resin and PVA had good adsorption for total bilirubin (TB), among them, NKA-9 ranked the top. Taken together, we considered the NKA-9 had the best adsorption for bilirubin from severe neonatal jaundice plasma.

3.2. Effects of NKA-9 on the Components of Severe Neonatal Jaundice Plasma
Under the experimental conditions, Table 1 listed the effect of NKA-9 on the components of severe neonatal jaundice plasma. According to the statistical analysis result, it showed that NKA-9 had insignificant effect on plasma biochemical parameters and also in line with basic clinical reference value.
3.3. Effects of NKA-9 on the Coagulation System of Severe Neonatal Jaundice Blood
Under the experimental conditions, Table 2 listed the effect of NKA-9 on the coagulation system of severe neonatal jaundice blood. According to statistical analysis, it showed that NKA-9 had insignificant effect on coagulation system indicators and also in line with basic clinical reference value.
3.4. Effects of NKA-9 on the Hemolytic System of Severe Neonatal Jaundice Blood
Under the experimental conditions, Table 3 listed the effect of NKA-9 on the hemolytic system indicators of severe neonatal jaundice blood. According to statistical analysis, it showed that NKA-9 had insignificant effect on hemolytic system indicators and also in line with basic clinical reference value.
4. DISCUSSIONS
According to the structure of bilirubin, the materials [17-20] currently reported to have better adsorption for bilirubin are mainly NKA-9, NK-110, PMMA, PVA, chitosan and burning resin. NKA-9 is a kind of macroporous resin with cyano, which has been mainly used in industry to extract bilirubin due to its good affinity to bilirubin; NK-110 is a kind of macroporous resin, which has been reported for the treatment of adult hyperbilirubinemia perfusion due to its good affinity to macromolecules toxic substances; PMMA also has adsorption for bilirubin, as well as good biocompatibility and blood compatibility, which has been widely used in biomedical materials field;PVA has been widely used in enzyme immobilization and blood purification fields in the form of membrane or water gel;Polysaccharide is a newly-developing adsorption and separation materials;Burning resin is an adsorption material from a variety of polymer resin produced by high-temperature carbonization.
This preliminary evaluation indicated the level of TB and DB in the severe neonatal jaundice plasma was significantly reduced after the plasma was hemoperfused by the six kinds of bilirubin adsorbing materials respectively, DB is a more important medical indicator for it reflects the function of liver. Among them, the adsorption of NKA-9 and PVA was the most significant; the adsorption ratio of NKA-9 was over 75%, and the adsorption ratio of PVA was over 50%. Although the level of TB and DB did not reduce to the normal level, the level had been below the threshold value of pathological neonatal jaundice (204-255µmol/L), which can help the doctors and the patients buy time to create favorable conditions for other treatments of neonatal jaundice. Regarding to the aspect of blood compatibility, NKA-9 resin did not cause significant effects on most of blood components indicators of newborn, and those indicators were also in line with the clinical reference value [20-21]. Inevitably, some indicators had significant change. For example, the level of HCO3- was below the normal value, which is adverse and unexpected in clinic treatment. However, such disadvantages can be easily remedied by other means. NKA-9 had major effects on the enzymatic system indicators of newborn, which is unexpected and need proper remedy. NKA-9 had little effects on the hemolytic system and blood clotting system indicators of newborn, which is favorable. Current studies [15,22] indicate hemoperfusion therapy for severe hepatitis is a good method for clearing bilirubin quickly. Due to hyperbilirubinemia becoming a common problem, therefore bilirubin adsorption therapy has great applicable prospect. In American, about 60% of 40 million neonatal may develop hyperbilirubina-emia [23], whereas 60% of hyperbilirubinaemia neonatal patients may develop into jaundice, of which pathological jaundice is higher than physiological one, whereas in China, incidence of pathological jaundice of newborn is up to 38.4% [24]. Because there still exist some drawbacks in current clinical therapies for pathological neonatal jaundice, improvements or new therapy is in urgent demand in order to gain great safety, therefore, how to cure neonatal jaundice (esp. the severe) with perfusion therapy and develop more effective, secure and economic bilirubin adsorbing material should be a novel challenge to the medical staff and scientists, and also has extensive market prospect. Unfortunately, the in vivo study cannot be now done because of the limitations of current technology.
5. CONCLUSION
The preliminary evaluations offer us the knowledge and reference of hemoperfusion being potentially applied in the treatment of severe neonatal jaundice; however, there still exists some problems to be resolved before it can be clinically used. Among six kinds of bilirubin adsorbing material candidates, NKA-9 resin had best adsorption for bilirubin from severe neonatal jaundice plasma, which may be expected as the adsorbing material to be used for the clinical hemoperfusion of neonatal jaundice disease with proper modification and therapeutic alliance. In future studies, people should develop new adsorbing material with high adsorption for bilirubin and with no/minor influences on other medical indicators except TB/DB, and/or seek compensative measurements to overcome the disadvantages causing by current bilirubin adsorbing materials.
ACKNOWLEDGEMENTS
This work was supported by the National Natural Science Fund(No.30900796) of China and the Doctor’s research initial fund of Henan University of Science & Technology China (No.09001284).