- Home
- About Journals
-
Information for Authors/ReviewersEditorial Policies
Publication Fee
Publication Cycle - Process Flowchart
Online Manuscript Submission and Tracking System
Publishing Ethics and Rectitude
Authorship
Author Benefits
Reviewer Guidelines
Guest Editor Guidelines
Peer Review Workflow
Quick Track Option
Copyediting Services
Bentham Open Membership
Bentham Open Advisory Board
Archiving Policies
Fabricating and Stating False Information
Post Publication Discussions and Corrections
Editorial Management
Advertise With Us
Funding Agencies
Rate List
Kudos
General FAQs
Special Fee Waivers and Discounts
- Contact
- Help
- About Us
- Search


The Open Arthritis Journal
(Discontinued)
ISSN: 1876-5394 ― Volume 7, 2014
Increasing Duration of Stationary Bicycling Does Not Increase Serum COMP in Subjects With and Without Joint Pathology
Timothy Cooney1, *, James DeLullo1, Michael Ghassibi 2, Ashlee Jones 3
Abstract
Objective:
Exercise has purported benefits for patients with osteoarthritis but dosing effects are not remarkable and poorly understood. We used serum levels of cartilage oligomeric matrix protein (COMP) to determine the effect of exercise duration on cartilage stress.
Methods:
Six men and 11 women, mean age 49.3 years (range: 25-69) who met inclusion criteria were enrolled with in-formed consent. The cohort consisted of those with (n=6) and without (n=11) joint pathology. Two separate bicycling ses-sions were conducted lasting 20 or 40 minutes. Session order was randomized. Pedaling resistance was adjusted to enable consistent speed (50 RPM) without exceeding 65% maximum HR. Venous blood, obtained before and after each session, was analyzed using a commercial COMP ELISA. Subjects also completed an AAOS Hip and Knee Outcomes Question-naire. Data were analyzed by repeat measures ANOVA and Pearson correlation.
Results:
After 20 minutes, mean COMP levels decreased from 811 ± 326.8 ng/ml to 768 ± 337.3 ng/ml; after 40-minutes,from 723 ± 311.8 to 693 ± 312.2 ng/ml. Neither duration of exercise or pathology significantly affected COMP. AAOS outcome scores were 83.7 (range: 65 to 94) for those with and 99.1 (range: 94 to 100) for those without patholo-gy/OA; scores did not correlate to COMP.
Conclusion:
Our data show that moderate, non-weight bearing exercise up to 40 minutes does not elevate serum COMP, suggesting it is to be non-injurious to joint cartilage for periods of this duration. Given the small subset of subjects with OA, additional study is warranted.
Article Information
Identifiers and Pagination:
Year: 2013Volume: 6
First Page: 1
Last Page: 5
Publisher Id: TOARTHJ-6-1
DOI: 10.2174/1876539401306010001
Article History:
Received Date: 14/1/2013Revision Received Date: 14/3/2013
Acceptance Date: 20/3/2013
Electronic publication date: 23/8/2013
Collection year: 2013
open-access license: This is an open access article licensed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted, non-commercial use, distribution and reproduction in any medium, provided the work is properly cited.
* Address correspondence to this author at the Orthopaedic Research Department, UPMC Hamot, 201 State Street, Erie, PA 16550, USA; Tel: 814-877-2684; Fax: 814-877-4010; E-mail: cooneyte@upmc.edu
| Open Peer Review Details | |||
|---|---|---|---|
| Manuscript submitted on 14-1-2013 |
Original Manuscript | Increasing Duration of Stationary Bicycling Does Not Increase Serum COMP in Subjects With and Without Joint Pathology | |
INTRODUCTION
Osteoarthritis (OA) is a degenerative disease that affects an estimated 27 million Americans or 12.1% of the adult population in the United States, making it the most common form of arthritis [1]. It develops primarily as a result of aging but other lifestyle variables such as obesity, cigarette smoking, and a history of manual labor have also been implicated [2]. Not only has the prevalence of osteoarthritis increased in the past six years, but the economic burden has as well. Medical expenditures for osteoarthritis and other arthritic conditions have increased from $233.5 billion in 1997 to $321.8 billion in 2003 [2]. As a result, over 900,000 total joint replacement surgeries were performed in 2009 at a cost of $42.3 billion [3]. OA, then represents a burden to the individual and society, as well.
Conventional methods for diagnosing and monitoring the progression of OA include both non-invasive/imaging and invasive/surgical studies. Typical radiographic signs of OA include joint space narrowing, subchondral bone sclerosis, and osteophyte formation. Direct visualization via arthroscopy represents the definitive method for assessing cartilage damage. Although both methods are staples for diagnosis, significant cartilage degradation has already occurred by the time the disease is detected.
Biomarkers have been proposed as a potential modality for early detection of arthritic changes. In particular, serum concentrations of cartilage oligomeric matric protein (COMP) have been shown to be elevated during periods of radiographic progression of the disease and are allied to disease stage [4-9]. COMP is a pentameric, non-collagenous glycoprotein which aids in chondrocyte mechanotransduction and collagen fibril formation [10,11]. These findings have led to additional research on this biomarker’s use as a prognostic and diagnostic indicator as well as a marker for disease severity and treatment effects [9].
In addition to diagnostic studies, COMP, along with other biomarkers, has been used to assess therapeutic effectiveness of conservative treatments for OA. Exercise has also been shown to allay pain and improve function in patients with OA [12-16]. Forms of exercise include aerobic, strengthening, aquatic, balance, and isometric exercise. Given that exercise involves joint loading, COMP levels are elevated after exercise in a manner commensurate to the degree of stress [17,18].
While exercise has shown to be beneficial for OA patients, little information is available, however, regarding effects of dosing, especially for patients with hip or knee osteoarthritis. As a starting point for understanding dose response, the present study monitored serum COMP levels immediately before and after stationary bicycling of two different durations in subjects with and without knee pathology. We hypothesized that levels of the biomarker would increase with increased duration of work, especially in the subset of patients with OA.
MATERIALS AND METHODS
Seventeen adult subjects, average age 49.3 years (range:25-69), were enrolled with informed consent in this repeated-measures, prospective, observational study. The average age was 49.3 years (range: 25-69; Table 1), and most were female (64%, 11/17). Six had either a history of knee or hip injury or a confirmed diagnosis of OA. Of these, all were female with an average age of 56.0 years (range: 33-69). Of the remaining eleven without pathology, the average age was 45.6 years (range: 25-61). Subjects were enrolled if they were between the ages of 18 and 80, were competent to perform stationary bike riding for up to 40 minutes and did not have a history of coagulopathies, cardiopulmonary disease, stroke, chronic infection or severe knee or hip OA (Kellgren-Lawrence Grade III or above). The study complied with the tenants of the Declaration of Helsinki and was approved by the hospital institutional review board.

The intervention consisted of two, stationary bicycling sessions for either 20 or 40 minutes performed on separate occasions but within a two-week period. The order of the sessions was randomized to preclude the effects of neuromuscular ‘learning’ for subjects with limited bicycling experience. Subjects were instructed to pedal at 50 RPM throughout the duration of the session. Pedaling resistance was adjusted to enable consistent effort without exceeding 65% of maximum heart rate. Either TRUE or Nautilus recumbent bikes were used in the study; both are products of Nautilus, Inc. (Vancouver, WA). To assess pain along with functional impairment, study subjects also completed the American Association of Orthopaedic Surgeons(AAOS) Hip and Knee Outcomes Questionnaire.
Prior to and within 30 minutes of the completion of each session, a 10-cc sample of venous blood was obtained from an antecubital vein. The timing of post-exercise sampling was performed to ensure peak serum levels [17,19]. Blood samples were centrifuged at 3,000 RPM for 10 minutes and the sera collected and stored at -80ºC until batch analysis. COMP assays were performed with a commercial ELISA (Biovendor, Chandler, NC).
Summary statistics were used to characterize the data. Repeated measures ANOVA was used to compare the effects of exercise duration and OA status on COMP levels. Pearson correlation was used to assess the strength of the relationship between AAOS outcome scores and post-exercise COMP levels. The threshold for significance was 0.05.
RESULTS
The average, standardized, mean AAOS outcome score for the cohort was 93.6 (range: 65-100). Mean score for the OA/joint pathology sub-group was 83.7 (range: 65-94) versus 99.1 (range: 94-100) for those without OA (p=0.020). AAOS scores were higher in the non-pathology (control) group (p<0.001), but failed to correlate with post-exercise COMP levels (p≥0.603).
Average COMP levels were 811 ± 326.8 ng/mlbeforeand 768 ± 337.3 ng/ml after a 20 minute exercise session (Table 2). Subgroup analysis revealed levels of 935 ± 345.6 before and 842 ± 332.0 ng/ml after 20 minutes of exercise in the joint pathology group (Fig. 1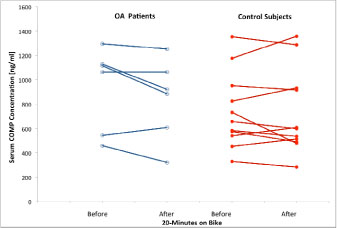 ); corresponding values for those without pathology were 744 ± 311.5 and 727 ± 349.1 ng/ml, respectively. For the 40-minute session, overall COMP levels were 723 ± 311.8 and 693 ± 312.2 pre- and post-exercise, respectively. For subgroup analysis, average COMP levels were 924.1 ± 287.1 before and 817.6 ± 372.4 ng/ml after exercise in the OA group (Fig. 2
); corresponding values for those without pathology were 744 ± 311.5 and 727 ± 349.1 ng/ml, respectively. For the 40-minute session, overall COMP levels were 723 ± 311.8 and 693 ± 312.2 pre- and post-exercise, respectively. For subgroup analysis, average COMP levels were 924.1 ± 287.1 before and 817.6 ± 372.4 ng/ml after exercise in the OA group (Fig. 2 ); for subjects without pathology, corresponding values were 631.4 ± 288.9 and 636.2 ± 281.8 ng/ml, respectively. Neither the duration of the exercise nor existing OA/joint pathology had an impact on COMP levels (p≥0.221). Post-exercise decreases in COMP levels were observed in approximately 70% of subjects with OA/joint pathology and 60% of those without.
); for subjects without pathology, corresponding values were 631.4 ± 288.9 and 636.2 ± 281.8 ng/ml, respectively. Neither the duration of the exercise nor existing OA/joint pathology had an impact on COMP levels (p≥0.221). Post-exercise decreases in COMP levels were observed in approximately 70% of subjects with OA/joint pathology and 60% of those without.


DISCUSSION
Our hypothesis was not supported. The data indicate that COMP levels did not become elevated when the duration of moderate intensity bicycling was doubled, from 20 to 40 minutes. Quite the contrary, more than half of the subjects manifested decreased levels after exercise (Figs. 1, 2), irrespective of duration. At baseline, the joint pathology group had a higher COMP level than controls but there was no difference between groups after exercise.

Pre-exercise COMP levels reported herein were consistent with values obtained by Jordan et al. [7]. They measured COMP levels of 806 ng/ml for individuals with no hip or knee OA (Kellgren-Lawrence stage 0) or 934 ng/ml for those with radiographic evidence of OA (Kellgren-Lawrence stages 2-4). In the present study, COMP levels were between 630 and 745 ng/ml in subjects without joint pathology and 924-934 ng/ml for those with a history of OA/injury.
Despite a large difference between mean values of COMP between subgroups, variability in the data coupled with small sample size mitigated against showing a statistical difference. Previous studies have shown differences in COMP levels as a consequence of ethnicity [7] and age [20]. However, COMP has shown its utility in many studies as a marker of joint stress along with its use as a quantitative marker for OA [4-9].
Contrary to our study, various weight-bearing exercise studies have reported increases in COMP following an exercise bout. A study by Kim et al. demonstrated that after running a marathon, there was 1.3-fold and 3-fold increase in the serum COMP levels for the 100 and 200 km marathons, respectively [21]. A follow up study by Kim et al. found a 1.9-fold increase in serum COMP at the end of the 200-km race. This elevated level of COMP was sustained for three days before returning to pre-race baseline levels on day six [22]. Niehoff suggested that mode of joint loading and intensity affect serum COMP concentration [23]. Aligned with this, our study limited patients to pedaling resistance that did not exceed 65% of maximum heart rate. Lack of a strenuous exercise protocol may have elicited less of a systemic change in serum COMP levels compared to previous studies.
To the extent that COMP levels reflect joint stress, our findings show a benefit for non-weight-bearing, moderate exercise. While surprising, this is not a unique observation. Recent studies by Helmark et al. have demonstrated increases in anti-inflammatory Interleukin-10 (IL-10) following bicycling as well as decreased intrasynovial COMP following a bout of leg extension exercise [24,25]. They found that exercise increases intra-articular and perisynovial levels of IL-10 in patients with osteoarthritis of the knee, whereas IL-10 remains unchanged in the non-exercise group. They proposed that these results suggest a positive effect of exercise on the expression of anti-inflammatory IL-10 in patients with knee OA and may contribute to the beneficial exercise effect on OA. Speculatively, the chondroprotective properties of IL-10 help suppress the release of inflammatory cytokines by macrophages. IL-10 was first identified as a cytokine produced by T helper type-2 (Th2) lymphocytes that strongly inhibit the production of pro-inflammatory cytokines IL-1, IL-6, IL-8, and TNA-α secreted by monocytes [26].
Other studies have documented the therapeutic benefit of exercise for patients with OA. A meta-analysis conducted by Bosomworth (2009) noted that moderate exercise for knee osteoarthritis helps reduce pain and disability along with improved physical functioning [27]. Fransen et al. went as far to say ‘the magnitude of the [exercise] treatment effect would be considered small, but comparable to estimates reported for non-steroidal anti-inflammatory drugs’[28]. In a more generalized sense, others have noted the positive role that exercise exerts on human articular cartilage [29,30]. Our data support these findings and suggest a biochemical basis for the therapeutic benefits of moderate exercise in patients with knee osteoarthritis. Our study was limited, however, by the small subset of subjects with joint pathology and the absence of standardized work intensity across the cohort.
CONCLUSION
Exercise prescription for patients with knee or hip OA has to consider the type of joint loading (including weight bearing), intensity, frequency and duration. The present study suggests that stationary bicycling up to 40 minutes does not cause an elevation in serum COMP levels. Given that COMP has been used as a biomarker of cartilage degradation, this study suggests that moderate, non-weight bearing exercise is not injurious to joint cartilage. Such exercise, performed at moderate intensity for up to 40 minutes, may actually hold potential benefit, especially in patients with existing joint pathology. Additional study is warranted.
CONFLICT OF INTEREST
This study was partially underwritten by a grant from the Lake Erie Consortium for Osteopathic Medical Training, Erie, PA, USA.
ACKNOWLEDGEMENTS
None declared.